The Three Factors That Determine Risk
Lesson 09 · Structural Decision Framework
In plain English
We see this all the time: two patients with the same X-ray, very different risk levels.
Both 50 years old. Both have a back molar with a moderate filling and slight wear. On paper, identical teeth. One needs a nightguard and a recheck in six months. The other can wait two years. The recommendation looks inconsistent until you see what we're actually weighing.
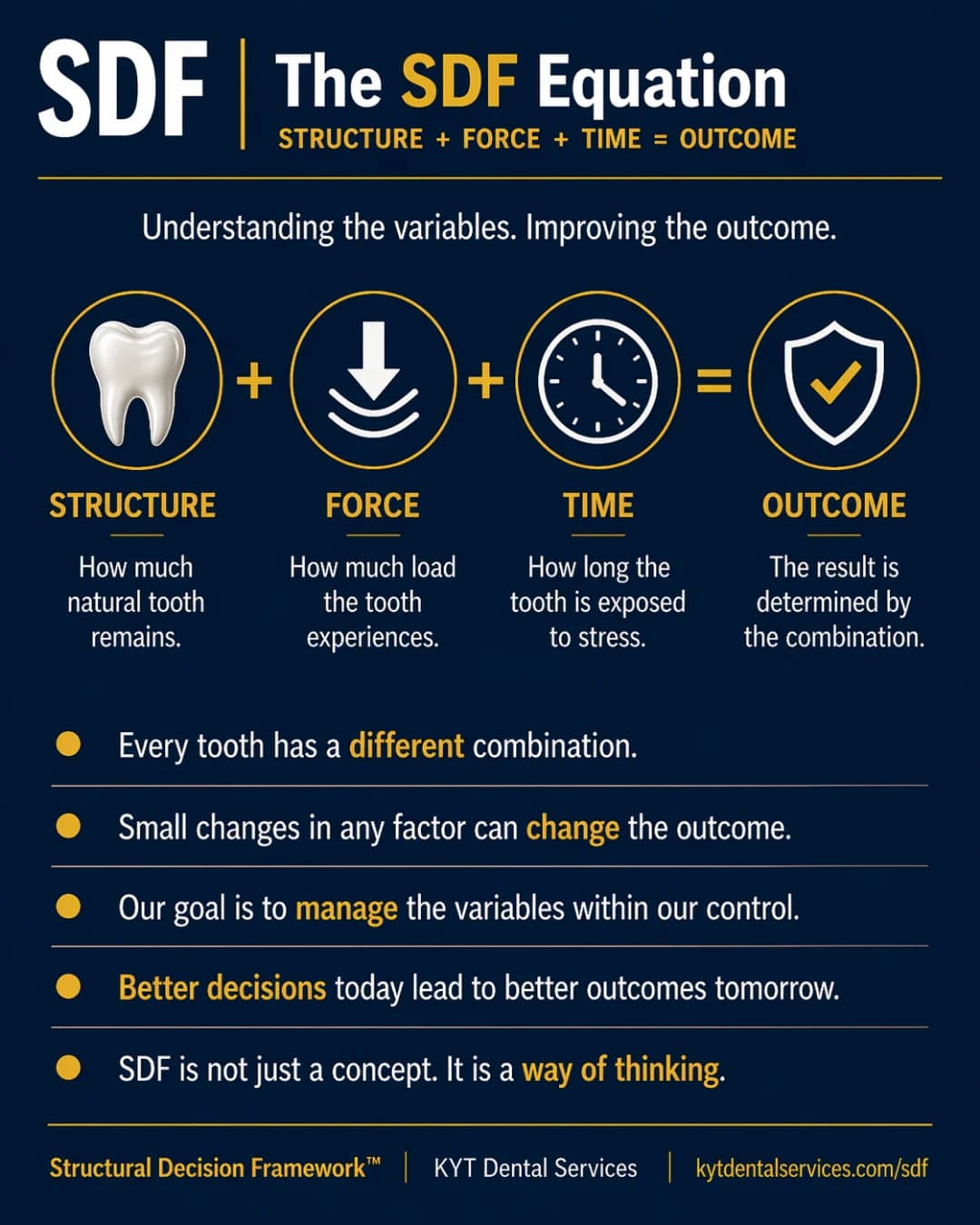
Risk in dentistry isn't random. It's an equation: structure × force × time.
Patient A grinds heavily at night. The structure is moderate, but force is high. The combination accelerates the math. They need intervention sooner, not because their tooth looks worse, but because their force profile is going to make it worse fast.
Patient B has a clean bite, no grinding, regular checkups. Same moderate structure, but force is low and time is well-monitored. The math runs slowly enough that watching is the right call.
This is the part most people don't realize about dentistry: the same finding can have completely different right answers in different mouths. Risk lives in the overlap of three variables, and the loudest variable is usually the one most worth fixing.
Structure is the hardest to change after the fact, which is why protecting it matters most. Force is usually the easiest to lower, a nightguard, a bite adjustment, addressing habits. Time can't be reduced, only watched. Most of dentistry comes down to identifying which of those three is loudest in your specific mouth, and acting where the leverage is.
When two patients walk out with different recommendations for what looks like the same tooth, the recommendations aren't inconsistent. They're following different equations.
The Lesson
One idea. One lesson.
Every idea in the Structural Decision Framework gets its own lesson. Hover to feel the foil.
SDF-09
StabilityThe Three Factors That Determine Risk

Tooth risk isn't random. It's structure × force × time, and the loudest of the three is usually the most worth fixing.
↓ Open the model
Inside the Model
Read the diagram.
Through the Stability lens, risk is the inverse of how stable a tooth is. The Three Factors That Determine Risk is the card that turns the abstract idea of stability into something you can act on: structure × force × time. The factor that's currently loudest is the one whose change buys you the most.
Fig. 09 · The Three Factors That Determine Risk
SDF Framework
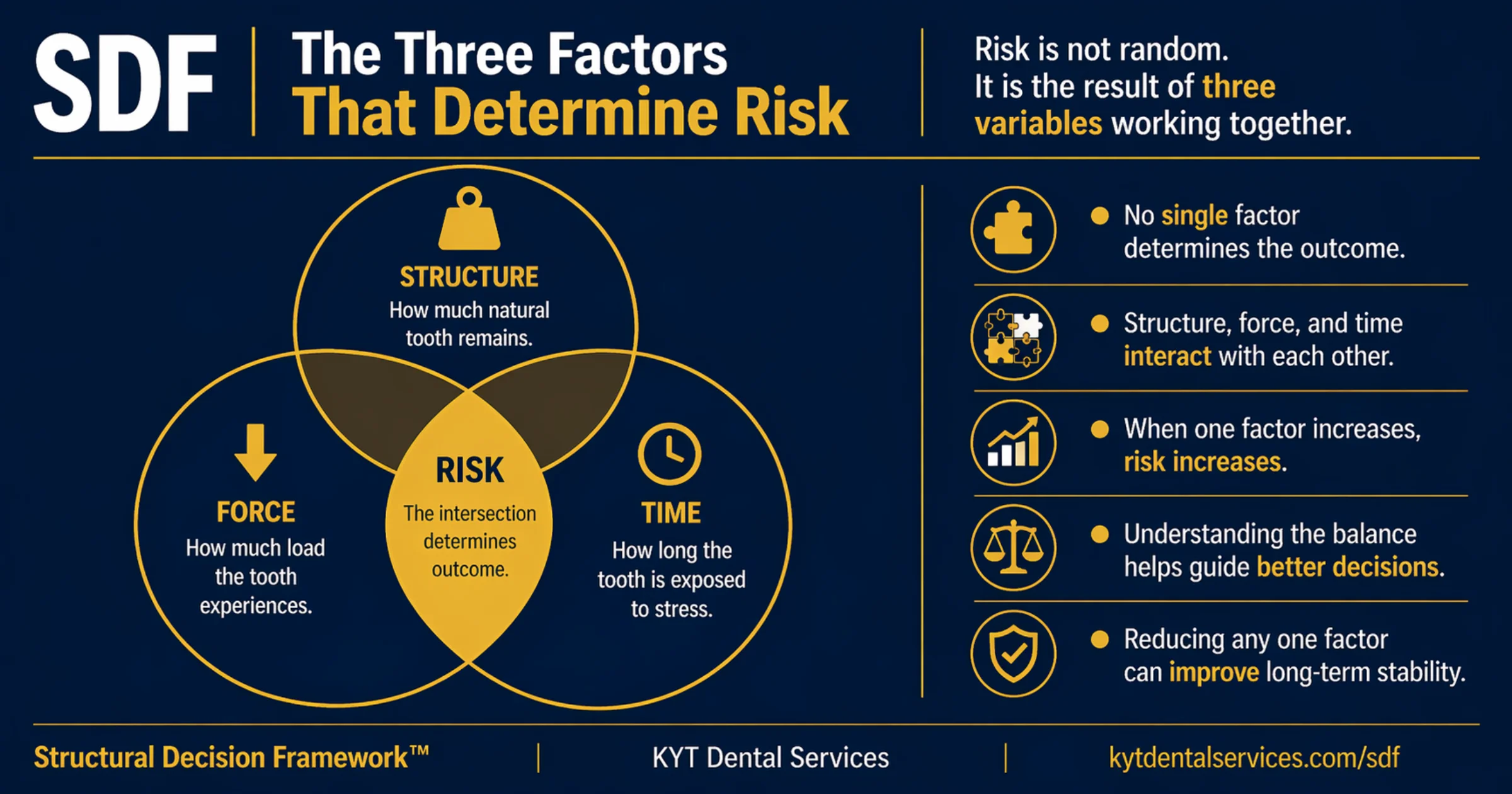
Risk isn't random. The chance a tooth has a problem in the next year, decade, or lifetime is the product of three things: how much natural structure is left, how much force is being applied, and how long the tooth has been under that pressure. Change one and the risk picture changes.
Explanation
Two patients can have the same tooth at the same age, and one is at high risk while the other is fine. The difference is almost never one factor; it's how three of them interact. Structure (how much real tooth is left after fillings, decay, or wear), force (how much load it takes, especially side-to-side), and time (how long the current load and structure combination has been running). Risk lives in the overlap. When all three are loud at once, risk is at its peak. Reduce any one, protect remaining structure with a crown, lower forces with a nightguard, catch problems sooner so time doesn't run out, and risk drops, even if the others stay the same.
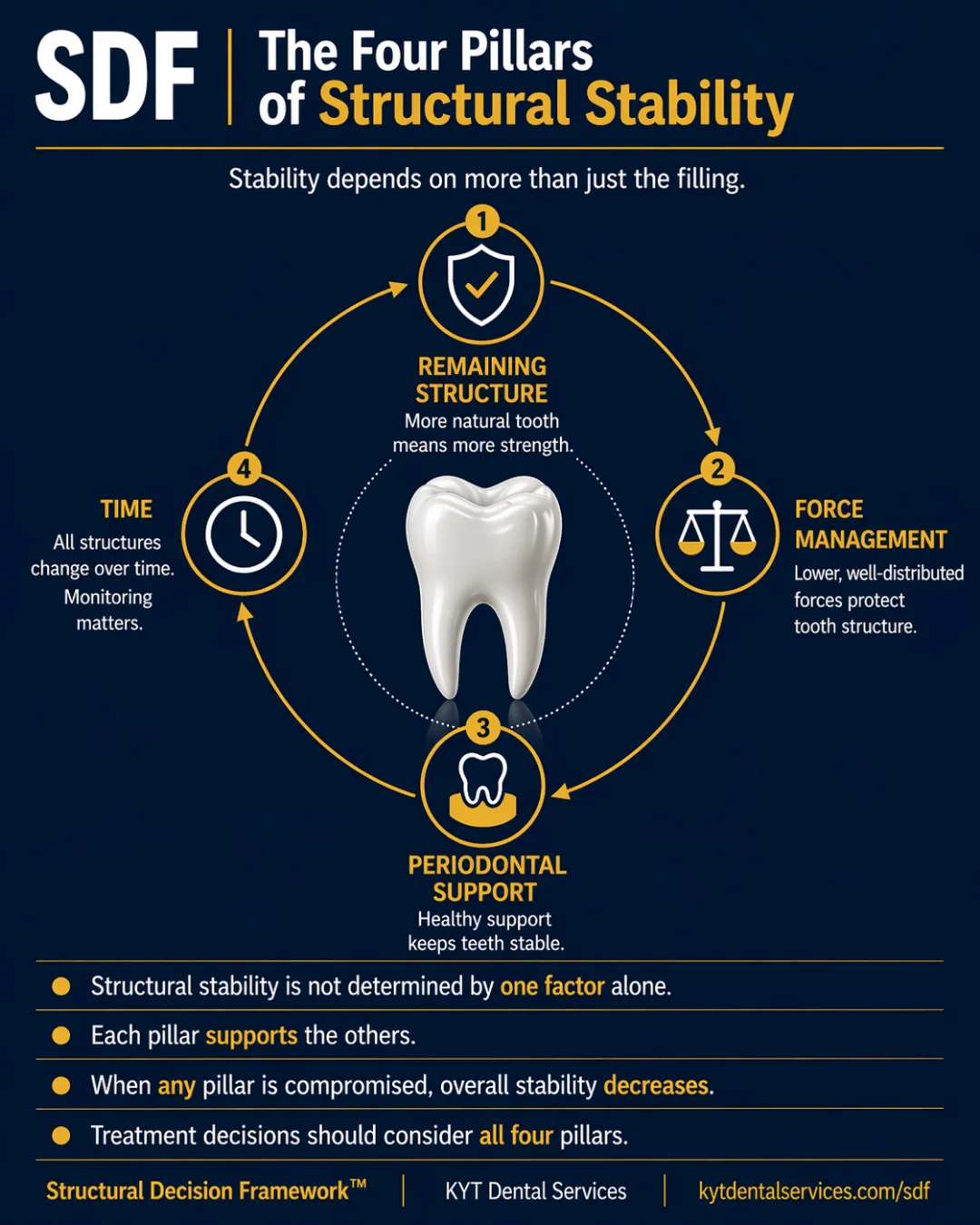
Key takeaways
- No single factor decides what happens to a tooth, it's structure, force, and time together.
- When any one of the three rises, risk rises. They don't cancel out.
- The three factors interact. A small problem on each is worse than one big problem alone.
- Understanding the balance is what makes treatment decisions targeted, not generic.
- Reducing the loudest factor is usually the highest-leverage move.
In the chair
How it shows up.
01
Same tooth, different patients
Two 50-year-olds with identical molars on X-ray. One has a nightguard and clean checkups every year. The other grinds untreated and skipped four years of cleanings. Same structure, very different force and time profiles. Same tooth, very different risk levels.
02
The fix that actually moves risk
A patient with low structural reserve (lots of fillings) and moderate grinding. Two options: another filling, structure stays the same, or a nightguard, which lowers force. The nightguard moves risk more, because force was the loudest factor. Treating the loudest factor wins.
03
The slow drift
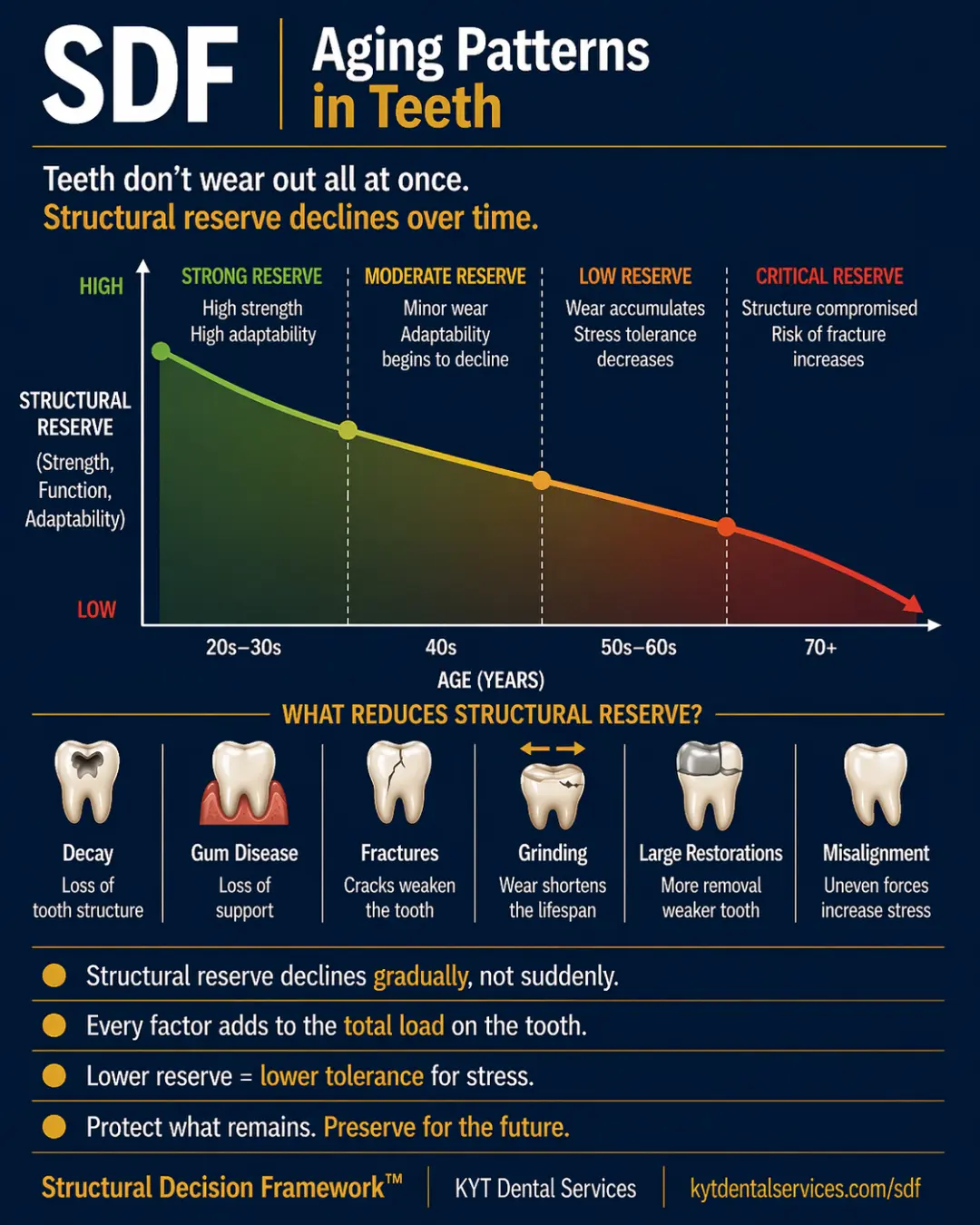
A young patient with full structural reserve, a normal bite, and good habits. Low risk now, but time is still ticking. Year over year, even minor wear accumulates. The reason for regular checkups isn't that something's wrong now; it's that time alone is one of the three factors, and watching it is how you catch it before it joins the others.
Through other lenses
The same idea, three other ways.
The first variable. Less natural tooth means less buffer against everything else. Structure is the hardest factor to change after the fact, which is why preserving it matters most.
The second variable. Bite, grinding, and side-load all add up. Force is often the easiest of the three to reduce, which is why nightguards and bite adjustments are so high-leverage.
The third variable. The longer a load has been on a structure, the more cumulative damage. Time can't be reduced, only watched and acted on early.
Common questions
FAQ.
How is risk different from damage?+
Damage is what's already happened. Risk is the chance more will happen, given what's there now. A tooth with a history of damage but a low current risk profile (structure preserved, low forces, well monitored) might be safer than a 'clean' tooth with high forces and no monitoring. Risk is forward-looking; damage is the historical record.
If I can only change one of the three, which is most impactful?+
It depends on which is currently loudest in your mouth. For grinders, lowering force is usually the highest-leverage. For someone with lots of old, large fillings, protecting remaining structure is. For most people, regular monitoring (treating 'time' as a factor to watch) is the constant baseline that keeps the other two from drifting.
Why do two people with the same fillings have such different outcomes?+
Because they're not actually the same, they have different force profiles (grinders vs non-grinders), different exposure times (years on the existing restorations), and different histories of structure preserved. Same tooth on the X-ray, very different risk equation.
Can risk drop, or only rise?+
It can drop. Reducing the loudest factor lowers risk even if the others stay the same. A nightguard reduces force; a crown protects structure; catching small things at checkups shortens the time damage has to run unchecked. Risk isn't a one-way street.
How does my dentist actually measure these three factors?+
Structure is read from X-rays and visible exam, how much natural tooth is left, how big restorations are. Force is read from wear patterns, bite analysis, and history (do you grind, clench, have an uneven bite?). Time is read from how long current restorations or wear patterns have been in place. Together, those three reads form the picture they're treating.
See it in real teeth
From idea to actual cases.
This site explains the idea. The clinical version, with real cases, real X-rays, and what this looks like in actual mouths, lives at KYT Dental Services, the practice this framework comes from.
See it on KYT Dental Services →Keep going